



Baseline characteristics and adherence to healthy lifestyles
From November 2014 to December 2021, a total of 531,683 participants with an elevated CVD risk were identified from the ChinaHEART project. We ruled out participants who underwent carotid ultrasound screening only once (n = 401,873), then excluded participants who had carotid plaque (n = 14,811) or CVD history (n = 15,975) at baseline, or had missing data for key variables (n = 20,553), or had a follow-up of more than 2 years (n = 34,717). Finally, a total of 43,651 participants were included in the study (Supplemental Fig. 1).
The mean age was 57.76 ± 7.95 years, and 27,288 (62.5%) were female. Overall, 29,296 (67.1%) participants lived in rural areas, 23,791 (54.5%) were farmers, 9,072 (20.8%) had received high school education or above, 5,532 (12.7%) participants had an annual household income above 50,000 yuan, 40,325 (92.4%) participants were married, and 42,255 (96.8) had social medical insurance. The average levels of SBP, blood glucose, TG, TC, LDL-C, and HDL-C were 157.00 ± 21.73 mmHg, 6.55 ± 1.85 mmol/L, 1.80 ± 1.07 mmol/L, 5.00 ± 1.29 mmol/L, 2.79 ± 1.09 mmol/L, 1.42 ± 0.44 mmol/L, respectively. The prevalence of overweight or obesity, hypertension, diabetes, and dyslipidemia was 69.6%, 45.1%, 25.7%, and 9.0%, respectively. 1.3% (557) and 27.8% (12,115) of the participants used statins and aspirin for primary prevention (Table 1).
Among the healthy lifestyles, none or moderate alcohol use had the highest adherence (n = 39,757, 91.1%), followed by non-smoking (n = 34,452, 78.9%) and sufficient LTPA (n = 13,932, 31.9%), while the adherence to a healthy diet (n = 4,209, 9.6%) was the lowest (Table 2). For multiple healthy lifestyles, there were 41,936 (96.1%) participants who adhered to at least one healthy lifestyle, while merely 3.6% adhered to all the four healthy lifestyles.
In the study cohort, 29,644 (67.9%) participants were at a high risk of CVD, while 14,007 (32.1%) were in the middle-risk group. Compared with those in the middle-risk group, participants in the high-risk group tended to be elderly, and were more likely to be male, living in rural areas, farmers, with lower education and income levels, with higher SBP, fasting glucose, and BMI, with history of hypertension and diabetes, as well as using statins and aspirin as preventive drugs (P < 0.05). They had lower adherence to none or moderate alcohol use and non-smoking, but higher adherence to sufficient LTPA (P = 0.006; Table 2). The proportion of participants who adhered to all the four healthy lifestyles was about the same in both middle- and high-risk groups (Table 2).
Association of healthy lifestyles with the incidence of carotid plaque
During a mean follow-up period of 1.74 ± 0.43 years, a total of 14,698 (33.7%) participants developed carotid plaque. There were 11,215 (37.8%) incidences of carotid plaque in the high-risk group, and 3483 (24.9%) in the middle-risk group, respectively.
According to the results of multivariable-adjusted logistic models, all of the four healthy lifestyles were separately associated with a lower risk of incidence of carotid plaque. The adjusted ORs (95%CIs) were 0.86 [0.80, 0.91] for non-smoking, 0.90 [0.84, 0.97] for none or moderate alcohol use, 0.94 [0.90, 0.99] for sufficient LTPA, and 0.90 [0.84, 0.97] for healthy diet. In the high-risk group, a lower risk of incidence of carotid plaque was associated with all healthy lifestyles, while the association disappeared in the middle-risk group. The interaction between middle- and high-risk groups was significant in sufficient LTPA (P for interaction < 0.05; Fig. 1, Supplemental Table 2).

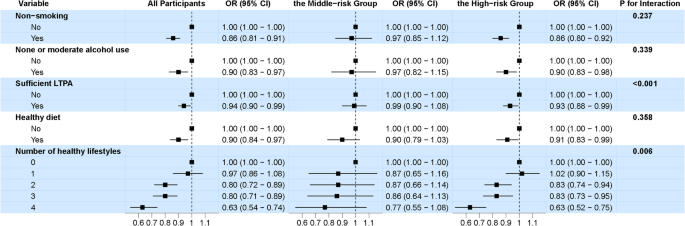
The association of healthy lifestyles with the incidence of carotid plaque. Note: LTPA = leisure-time physical activity
When the healthy lifestyles were combined, a significant inverse linear relationship was observed between the number of healthy lifestyles and the risk of incidence of carotid plaque (P for trend < 0.001). Compared with those adhering to none of the lifestyles, participants who adhered to all four healthy lifestyles had the lowest risk of incidence of carotid plaque (OR: 0.64 [0.54, 0.75]). The association was stronger in the high-risk group than in the middle-risk group (0.63 [0.53, 0.76] vs. 0.78 [0.56, 1.10]), P for interaction < 0.05; Fig. 1, Supplemental Table 2). Moreover, the synergistic effect of the four healthy lifestyles on preventing carotid plaque was significant (P for interaction < 0.001).
Subgroup analyses showed that elder participants, those living in urban, and non-farmers, as well as those having lower income levels benefited more from adherence to healthy lifestyles, compared with their counterparts (P for interaction < 0.05; Table 3).
Association of healthy lifestyles with the incidence time of carotid plaque
According to the results of multivariable parametric AFT models, a postponed incidence time of carotid plaque was associated with non-smoking (TR: 1.06 [1.03, 1.08]) and healthy diet (1.04 [1.01, 1.06]). In the high-risk group, the adjusted TRs (95% CIs) were significant in non-smoking (1.05 [1.02, 1.08]) and healthy diet (1.03 [1.00, 1.06]), while in the middle-risk group, no significant postponed time of carotid plaque was seen in any healthy lifestyles. The interaction between middle- or high-risk groups was significant in terms of sufficient LTPA (P for interaction < 0.05; Fig. 2, Supplemental Table 3).

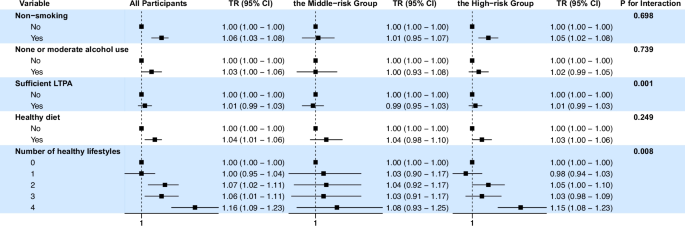
The association of healthy lifestyles with postponed incidence time of carotid plaque. Note: LTPA = leisure-time physical activity
When the healthy lifestyles were combined, the number of healthy lifestyles was largely positively associated with the delay of plaque incidence time. Compared with those who adhered to none of the lifestyles, participants who adhered to all four healthy lifestyles had the longest delay of plaque incidence time (1.16 [1.09, 1.23]). The association was stronger in the high-risk group than in the middle-risk group (1.15 [1.08, 1.23] vs. 1.08 [0.93, 1.25]), P for interaction < 0.05; Fig. 2, Supplemental Table 3).
Subgroup analyses showed that, among all participants, the elderly, those living in urban areas, and non-farmers benefited more from adherence to healthy lifestyles than their counterparts. (P for interaction < 0.05; Table 3).
Mediation analysis and sensitivity analysis
In the mediation analysis, the relationship between healthy lifestyles and the risk of carotid plaque was mediated by SBP, fasting glucose, TG, TC, and HDL-C with the proportion of mediation effect ranging from 1.5% to 7.9% (Supplemental Table 4).
The sensitivity analysis results were generally consistent with the main analysis. Notably, participants’better adherence to healthy lifestyles was associated with lower risk of carotid plaque and longer time to plaque formation. Details of the sensitivity analyses are presented in Supplemental Table 5 and 6.
link